Emmetropia is the state of vision where a distant object at infinity remains in sharp focus with the eye lens in a neutral or relaxed state. This condition of the normal eye is attained when the refractive power of the cornea and the axial length of the eye balance out, which focuses rays exactly on the retina, leading to twenty-twenty. A human eye in a state of emmetropia needs no corrective lenses; the vision scores well on a visual acuity test (such as an eye chart test). For example, on a Snellen chart test, emmetropic eyes score at “6/6″( m) or “20/20″( ft) vision, whereas myopic (near-sighted) eyes might score at 20/40 and hyperopic (far-sighted) eyes may score at 20/15.
“Emmetropia” is originated from Greek ἔμμετρος emmetros “well-proportioned” (from ἐν en “in” and μέτρον metron “procedure”) and ὤψ ōps “sight” (GEN ὠπός ōpos). Translated literally, the term shows the condition of an eye’s having in itself (i.e., without recourse to restorative lenses or other instruments) the ability to obtain an accurate measurement of a things’s physical look.
What Is Emmetropia?
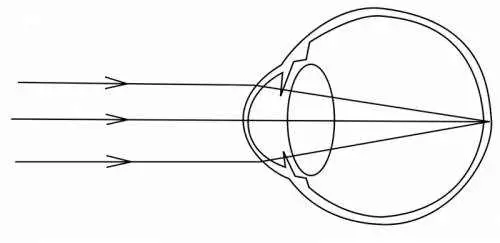
Emmetropia is a state where the eye is relaxed and concentrated on an item more than 6 meters or 20 feet away. The light rays originating from that object are basically parallel, and the rays are concentrated on the retina without effort. If the gaze shifts to something better, light rays from the source are too divergent to be focused without effort. In other words, the eye is immediately focused on things in the distance unless a mindful effort is made to focus somewhere else. For a wild animal or human prehistorical ancestors, this plan would be adaptive since it allows for alertness to predators or prey at a distance.
Vision Support: Quality AREDS 2 Formula eye vitamins can be found on Amazon.
Accommodation of the lens does not happen in emmetropia. In emmetropia, the lens is about 3.6 mm thick at the center; in accommodation, it thickens to about 4.5 mm. A reasonably thin lens and fairly dilated pupil are also associated. The lens usually stiffens with age, causing less ability to focus when the eyes are not in a state of emmetropia.
Restorative eye surgery such as LASIK and PRK intends to fix anemmetropic vision. This is accomplished by guaranteeing the curvature of the cornea, the shape of the lens and their ranges from each other and the retina agree. By forming the cornea, emmetropic vision can be attained without corrective lenses. The correction for just emmetropic vision is typically why patients are still encouraged to wear glasses to read as they age due to presbyopia.
Newborns begin hypermetropic then undergo a myopic shift to become emmetropic.
Emmetropization
The development of an eye to emmetropia is referred to as emmetropization. This process is assisted by visual input, and the mechanisms that coordinate this process are not fully comprehended. It is presumed that emmetropization takes place by means of an active mechanism by which defocus drives growth of the eye which hereditary aspects and emmetropization both influence the growth of the eye’s axis.
There has actually been some research on causal factors involved in the advancement of myopia and of hyperopia. In particular, stats show that prolonged near work associates with the development of myopia, however it is still uncertain whether there is a causal relation. In addition, outside activity has been discovered to have a protective effect on myopia advancement in children.
Expert Choice: Recommended by eye care professionals for managing dry eyes, styes, and blepharitis, this Heated Eye Mask provides the consistent moist heat therapy endorsed by the American Academy of Ophthalmology. It’s an effective, reusable solution for soothing irritation and improving oil gland function. Available on Amazon.
It has long been assumed that wearing restorative eyeglasses might perhaps alarm the procedure of emmetropization in young kids, with this presumption being supported in particular likewise by animal studies. For this reason, a refractive undercorrection is sometimes held to be advantageous in particular cases. However, it is not yet fully comprehended for which patient groups, if any, the wearing of restorative eyeglasses in youth really impedes emmetropization. In hyperopic children, yet more factors are to be considered: Hypertropia is known to be a considerable risk element for esotropia, therefore undercorrection might have the side effect of increasing this risk.
There is widespread consensus that undercorrection is counterindicated for children with accommodative esotropia. It is still uncertain for which hyperopic, non-strabismic children corrective eyeglasses may equate to a lower strabismus risk. There are signs that emmetropization matters for hyperopic children who have at the majority of about 3.0 diopter, whereas children with stronger hyperopia appear to not change their refraction separately of whether the refractive mistake is fixed or not.
Specialized Care: For persistent itching or flaking, eye care specialists recommend targeted formulas like this BetterLids Eyelid Ointment . This preservative-free, dermatologist-tested oat complex is a top choice for soothing sensitive skin and managing symptoms of blepharitis. Available for easy ordering on Amazon.
A Cochrane Review of 3 trials seeking to identify whether spectacle correction lowered the incident of strabismus in children consisted of one study which suggested that spectacle correction worried emmetropization in children, while a 2nd research study reported no differences.


